Ankle Instability
Background
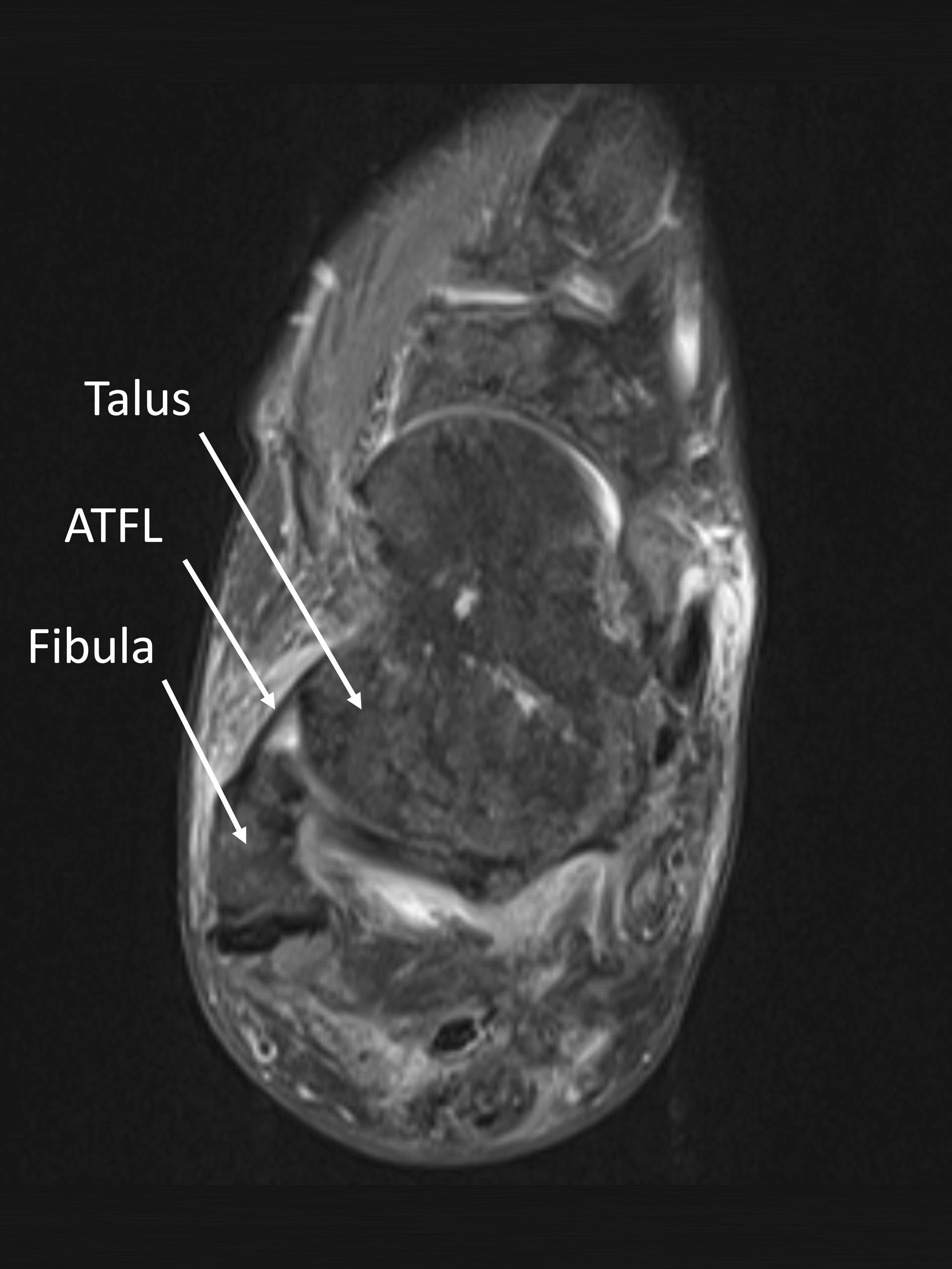
The primary stabilizer of the ankle joint is the anterior talofibular ligament (ATFL). This ligament connects the tip of your fibula to the talus, effectively connecting your leg bones to your foot bones. This is the ligament that prevents you from turning your ankle inward (inversion), which is the most common mechanism of ankle sprain.
In a severe ankle sprain, the ATFL becomes completely ruptured and your ankle becomes unstable. After a severe ankle sprain, with proper treatment (immobilization followed by focused physical therapy), the ATFL should reform from scar tissue to restabilize your ankle. However, if you sprain your ankle repeatedly (for example, more than once per year), the ATFL grows back in a weaked and attenuated fashion. As you can imagine, this becomes a cyclical problem, with the weakened ATFL predisposing to additional ankle sprains, and additional ankle sprains further weakening the ATFL.
When the ankle becomes chronically unstable and ankle sprains become recurrent and common, the cartilage can become damaged within the ankle joint as well. This can lead to additional pain and even the development of early arthritis.
Recurrent ankle sprains are common among young people and athletes. They can become debilitating for sports participation, as the weakened ankle is unable to cut or pivot, and the ankle may become painful even with in-line motion. If any of this describes your situation, you can certainly benefit from evaluation and treatment.
Diagnosis

At your foot and ankle sports consultation, Dr. Bohl will examine all the ligaments, bones, and muscles below the knee. If you report recurrent ankle sprains, Dr. Bohl will pay particular attention to the ligaments of the lateral ankle, in particular the ATFL. Specific physical examination maneuvers will elicit pain, weakness, or laxity of this ligament.
Dr. Bohl will always obtain x-rays of your foot and ankle as well. These will demonstrate whether any bony damage or early arthritis has developed. If your ankle pain is chronic and you have tried at least some initial forms of managing your pain (anti-inflammatories, rest, ice, stretching, etc.), then Dr. Bohl will recommend an MRI of your ankle.
MRIs are a powerful tool for clarifying ankle instability. Most importantly, an MRI will demonstrate evidence of weakening, laxity, attenuation, and chronic injury to the ATFL. An MRI will also demonstrate whether the cartilage or peroneal tendons have been concurrently injured, and whether they should be concurrently addressed.
Nonsurgical management
Treatment always begins with nonsurgical management. For chronic ankle instability, this involves a lace-up ankle brace and physical therapy.
The lace-up ankle brace provides restraint against inversion and also a sort of sixth sense to the body wherein your ankle more easily detects and acts to prevent an inversion injury. Taping by a physical therapist or athletic trainer prior to sports participation can have a similar effect.
Physical therapy is encouraged and serves to strengthen the dynamic stabilizers of the lateral ankle so that these muscles can tighten in the event of an inversion moment to prevent a full-on recurrent sprain. Many patients are able to improve to the extent of avoiding surgery with these interventions.
Surgical management


For many patients, no matter how much physical therapy and bracing are performed, the ankle pain and/or sprains continue to occur. Fortunately, there are excellent surgical solutions for ankle instability.
Dr. Bohl recommends that most patients with chronic ankle instability who have failed nonsurgical management undergo concurrent ankle scope and reconstruction of the ATFL:
First, through two tiny poke holes on the front of the ankle, instruments including a camera are inserted into the ankle joint. The cartilage is inspected and any defects to the cartilage or the underlying bone are treated. This part of the procedure is similar to treatment of an OCD, which is described in detail here. Any synovitis, or articular inflammation, is also removed, which can be important for pain relief.
The second part of the procedure is the reconstruction of the ATFL, to provide stability and prevent additional sprains. Dr. Bohl performs a “modified Brostrum” procedure, which is the most tried and true method of restoring stability to the lateral ankle. In this procedure, the ATFL is tightened back up to suture anchors placed within the tip of the fibula. The stability is then evaluated intraoperatively with physical examination manuvers. For most patients, the modified Brostrum is sufficient. However, for those with severe laxity and/or previous surgery for the same issue, Dr. Bohl recommends augmentation with the Internal Brace.
After surgery, patients are placed in a splint for 2 weeks, followed by a cast for 4 weeks, followed by a boot for an additional 4 weeks. Weight bearing is allowed when the cast comes off. During those first 6 weeks. Dr. Bohl recommends use of a rolling knee scooter. Patients do extremely well after reconstruction of the ATFL; of course the plan is for a full return to athletic activities.
Revision procedures
Unfortunately, Dr. Bohl commonly sees patients in his clinic who have previously had ATFL reconstructions that have failed. Such patients may experience recurrent instability, additional sprains, chronic pain, or early arthritis. These can become complicated cases requiring augmentation with autograft or allograft in order to restore stability, and/or complex cartilage reconstructive procedures.
In these cases, your prior operative reports, MRI images, and MRI radiology reports are all critical for complete evaluation — please hand carry these all with you to clinic. After a physical exam and full review of your imaging, operative reports, and personal goals, Dr. Bohl will be happy to discuss the risks and benefits of revision reconstruction.